Leaving the hospital
When you are well enough to leave our care, we’ll make sure you have what you need to go home. A medical provider will write your discharge orders, instructions and any prescriptions for medicines you may need. The nurse will give you a printed copy of the information and discuss it with you and your loved ones before you go. We encourage you to ask any questions or address concerns you may have at that time.
Follow-up call at home
If you are returning home, a nurse from Salem Health may call you within the first several days to see how things are going. These discharge callers are a special team that review medicines and discharge instructions with you and answer specific questions that may have come up after you leave. Please share your concerns and ideas on how we may improve.
Social services and care management
Your care management team includes nurses, social workers, and associates who are specifically trained in care coordination and transition planning. At Salem Health, care managers are available at every inpatient unit, the emergency department and many of our clinics.
You, or your designated health care representative, have the right to:
- Be educated about your ongoing health care.
- Be involved in the planning and coordination of your ongoing health care.
- Choose which agencies or facilities provide your ongoing health care.
Along with all the members of your Salem Health treatment team, your care managers are:
- Available to help you navigate the complex system of services, compatible insurance coverages and discharge arrangements.
- Here to advocate for you.
At Salem Health, transition planning begins the moment you become a patient. As your health care needs change, care managers continually work to review your health care challenges to help you consider services you might need and/or qualify for.
Services your care management team provides:
- Screening of needs, which may include: a comprehensive psychosocial assessment, coordination with all providers, and timely facilitation of appropriate resources.
- Supportive, brief counseling.
- Developing alternative level of care plans.
- Education about illness, support for coping, resources and services.
- Community resource information: financial assistance, medication, counseling, support groups, housing, and transportation.
- Advocacy and support.
- Navigating the health care system.
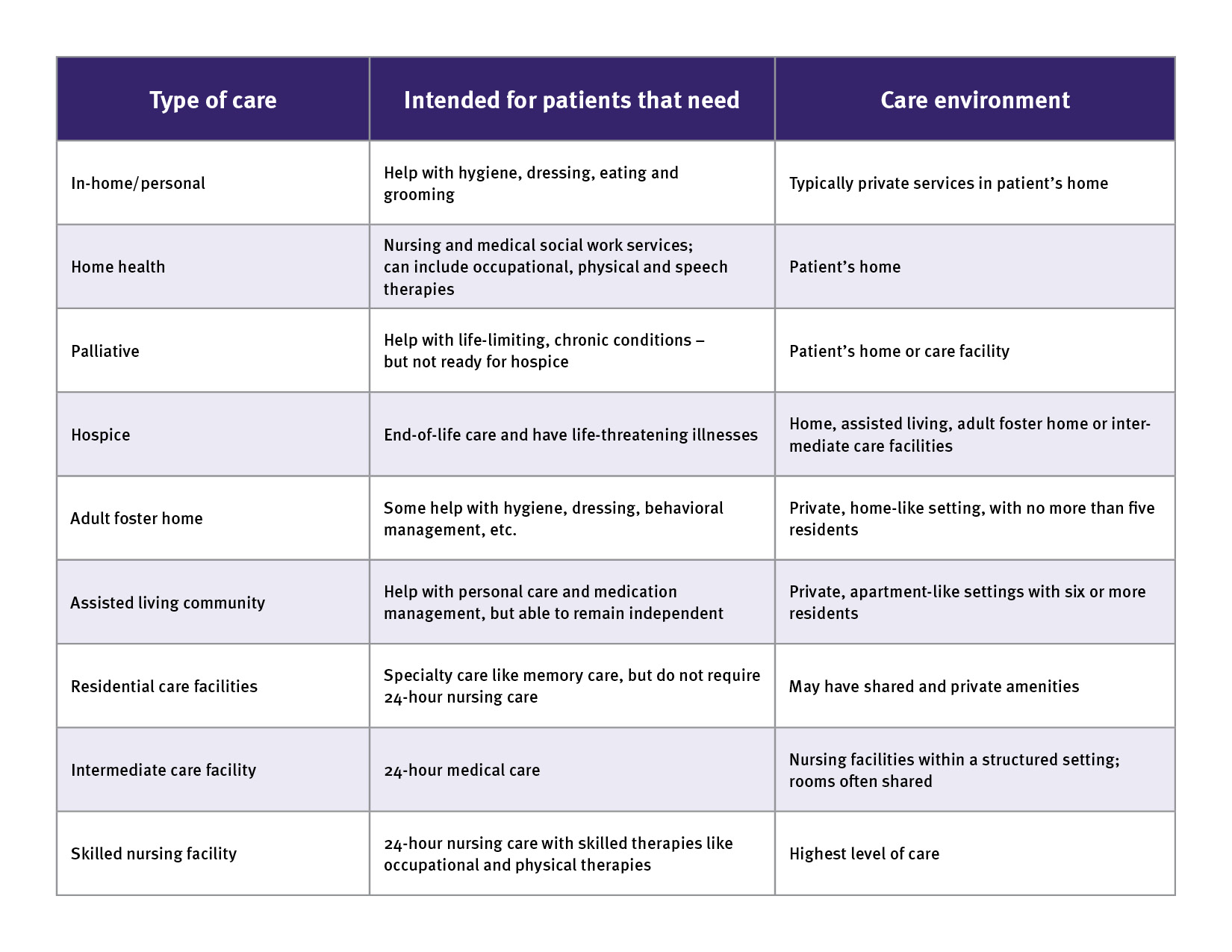
Short and long-term care planning services may be funded by federal, state, or local entities, or you may need to pay for them privately. Your care manager can help explain the differences.